
Allocation Out of Sequence (AOOS)
Additional resources about AOOS are available here:
AOOS Workgroup AOOS FAQs
Improving allocation practices to strengthen public trust and patient outcomes
The Organ Procurement and Transplantation Network (OPTN) creates, implements, and monitors national policies that describe how donated organs should be allocated to patients waitlisted for a transplant. Laws, regulations, and policies require that organs are allocated fairly, transparently, and according to the criteria the OPTN establishes. Allocation Out of Sequence (AOOS) occurs when OPTN members allocate organs outside of the OPTN-designed match run; generally, these AOOS actions do not comply with OPTN allocation policies, resulting in patients losing their opportunity to receive an organ to which they were matched. As the OPTN modernizes, HRSA and the OPTN are committed to addressing AOOS to protect public trust, ensure the policies that the OPTN designs and enacts are followed, and uphold patient safety.
What is AOOS?
The OPTN, as directed by HRSA, developed shared operational and analytic definitions describing organs allocated out of sequence.
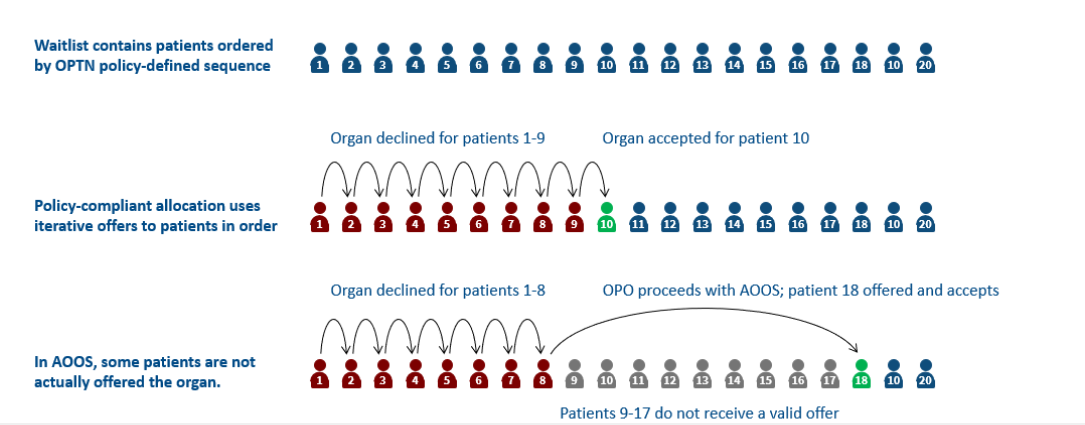
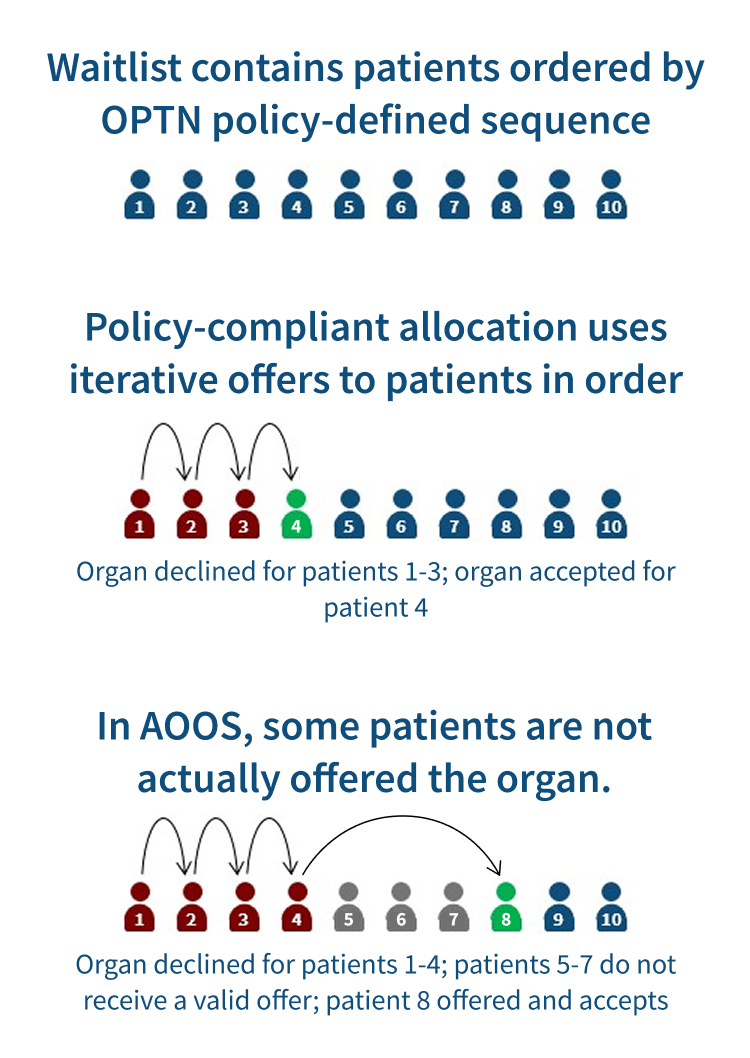
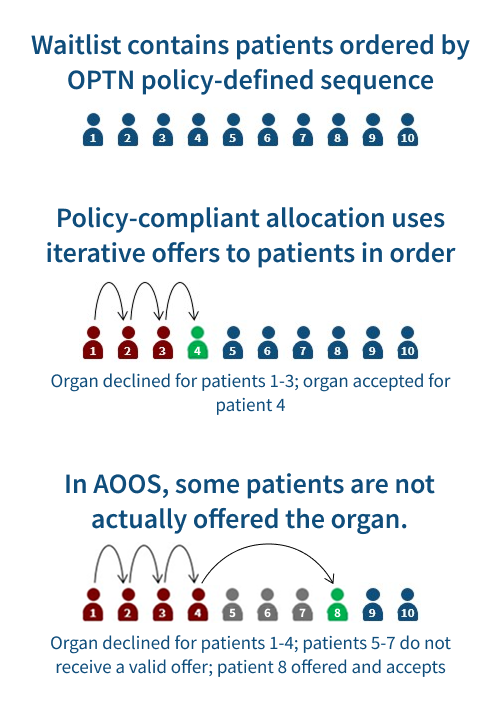
AOOS is when an organ is offered or accepted or transplanted into a transplant candidate or potential transplant recipient (PTR) that deviates from the match sequence and is not consistent with OPTN policy.
AOOS is identified through the use of one or more of the following organ offer bypass codes:
- 861: Operational - Organ Procurement Organization (OPO)
- 862: Donor medical urgency
- 863: Offer not made due to expedited placement attempt
- 887: Not Offered - expedited placement
- 799: Other (specify)
Example of AOOS
What about “wasting” a donated organ?
The OPTN Final Rule provides a policy-compliant way to ensure that, in emergencies or unintended disruptions, an organ allocated to a patient at a transplant center may be emergently used in another suitable patient. While some stakeholders have expressed a hope that non-compliance with the OPTN allocation policies prevents wasting donated organs, in practice, organ non-use has gone up as AOOS has also risen.
The OPTN was advised by HHS that the “wastage provision at 42 CFR 121.7(f) [does not] authorize out-of-sequence offers by OPOs. This provision on its face provides authority to transplant centers to determine that organ recipients should be identified other than in accordance with 121.7 and OPTN policies and procedures and does not provide this authority to OPOs. And insofar as transplant programs rely on this provision to justify out-of-sequence placements of organs, we believe they may only do so to the extent that the organs would otherwise go to waste.”
Organ allocation, under requirements of the Final Rule and OPTN Bylaws and Policies, is required to be fair, offer organs not to transplant centers but instead to potential recipients, be ranked by priority, and be sequentially offered to potential recipients.
See more about how donated organs are matched to potential recipients here.
Why does AOOS raise concerns?
AOOS poses serious risks and consequences:
- It may violate federal laws and policies, including the National Organ Transplant Act (NOTA), the Final Rule, and OPTN policies and bylaws.
- It can lead to patients being unfairly bypassed, denying them potentially life-saving transplants.
- It can damage public trust in the integrity, transparency, and fairness of the organ procurement and transplant system.
Accountability to patients is fundamental to meaningful OPTN modernization. Adherence to established policies is not optional. In fact, it is the foundation of accountability. Ensuring this accountability protects patients, supports health providers, and preserves the credibility of the national procurement and transplant system.
What can we learn from data?
While analyses of AOOS will continue and evolve moving forward, early findings reveal several important trends:
- AOOS is occurring across multiple organ types and regions, suggesting it is not limited to a specific organ system or geographic area.
- Candidates who meet established priority criteria may still be bypassed, raising concerns about fairness in the allocation process.
- Limited transparency around AOOS is causing uncertainty and concern among both patients and healthcare providers.
These initial insights highlight the urgent need for greater data transparency and policy clarity.
In 2024, 19% of organ allocations were AOOS. Explore how AOOS and organ non-use rates have varied over time and across organ procurement organizations (OPOs):
For issues viewing the dashboard, please click here to access the dashboard.
For dashboard questions, please contact AskDOT@hrsa.gov.
HRSA and the OPTN are committed to data transparency and accessibility. With HRSA’s support, the OPTN is developing a consensus, living dataset for the community to use in AOOS analyses; when that dataset is available, these graphs and the details below will be updated accordingly.
Please contact AskDOT@HRSA.gov with questions about this analysis or suggestions for how to improve future versions of this dashboard.
Allocation out of sequence
- This graph shows the percent of organ allocations that met the OPTN’s analytic definition of AOOS.
- The “All OPOs (Median)” line shows the median AOOS rate by OPO for each month. The individual OPO lines show a rolling average over the previous six months. To protect patient privacy, data points that would be calculated from fewer than 15 total allocation events are not shown.
- The full organ donation, procurement, and transplant process can take several days. In this graph, the date of an organ’s allocation is counted as the date when an OPO executed a match run to determine the sequence of potential recipients who would be offered that organ.
- An allocation is considered out of sequence if one or more of the AOOS organ offer bypass codes was recorded for a potential transplant recipient ranked earlier on the match run than the patient who accepted the organ. An allocation is not considered out of sequence if AOOS bypass codes are present only at later sequences than the patient who accepted the organ. (Note that in rare cases, the patient who accepts the organ may not be the patient who receives the transplant.)
- Sometimes more than one refusal or bypass code is entered in response to a single organ offer. This analysis considers the latest code entered for each offer, which may have been recorded by an OPO, a transplant center, or the OPTN computer system.
- OPOs are required to report organ offer outcomes, including bypass codes, within 30 days of the match run date. (See OPTN Policy 18.3 for more detail.) Because data are largely incomplete within this 30-day reporting period, this graph shows results with a one-month delay from the date of analysis.
- Sometimes an OPO runs more than one match run for the same organ(s). In this analysis, most allocations are counted once per organ:
- If the organ was transplanted, we count the match run used to allocate the organ for transplant.
- If the organ was accepted but not transplanted, we count the latest match run on which it was accepted.
- Organs that were offered but neither accepted nor transplanted are not included in this graph because offers cannot be characterized as in or out of sequence using existing OPTN allocation data.
- Multi-organ transplants allocated on a single match run are counted as a single allocation event. For example, if a recipient is allocated a lung on a lung match run and also receives a kidney from the same donor as part of a multi-organ transplant, that allocation is counted once.
- Separately transplanted organs allocated on the same match run (for example, two kidneys from the same donor into separate recipients) are counted as separate allocation events.
- This analysis includes the following organs: kidney, pancreas, liver, intestine, heart, lung. This analysis excludes islet cell and vascularized composite allotransplantation (VCA) transplants.
- This analysis only includes organs procured and transplanted in the U.S. From 2015 to 2024, an average of <10 organs per year were procured outside the U.S. and transplanted in the U.S.
- An allocation event is counted for the OPO that submitted the match run, even in rare cases where this is not the same OPO that performed the procurement surgery.
Organ non-use
- This graph shows the proportion of all organs procured for transplant that were not ultimately transplanted.
- The “All OPOs” line shows the median organ non-use rate by OPO for each month. The individual OPO lines show a rolling average over the previous six months. To protect patient privacy, data points that would be calculated from fewer than 15 total allocation events are not shown.
- The full organ donation, procurement, and transplant process can take several days. In this graph, the date of an organ’s use or non-use is counted as the date of the organ recovery surgery.
- An organ use/non-use event is counted for the OPO that performed the procurement surgery, even in rare cases where a different OPO executed a match run for that organ.
What actions are being taken to address AOOS?
The OPTN is working to ensure that organ allocation is fair, transparent, and in line with national policy by:
- Ensuring all organ allocation follows laws, regulations, and OPTN policies
- Limiting AOOS to rare, well-justified, and transparent exceptions
- Strengthening fairness and rebuilding public trust in the procurement and transplant system
- Collaborating with stakeholders across the OPTN community to ensure that different perspectives, especially those of patients and their families, are represented
Progress is already underway:
- An AOOS Workgroup was formed that is composed of representatives from multiple OPTN committees, including, but not limited to, the Patient Affairs Committee (PAC), Data Advisory Committee (DAC), Ethics Committee, and Membership and Professional Standards Committee (MPSC) to implement the AOOS Remediation Plan.
- The OPTN operations contractor, as directed by HRSA, developed drafts of queries that can be run against raw OPTN data to produce a consensus, living dataset for the analysis of AOOS. In response to these drafts, HRSA requested input from the OPTN on several foundational characteristics of the consensus dataset. When finalized, this dataset will be updated regularly with new records and made available, under appropriate data use agreements, to any transplant community member interested in the issue of allocation policy noncompliance.
- HRSA reviewed and provided feedback on the OPTN’s draft AOOS Remediation Plan to strengthen national allocation policy and clarify definitions.
- The OPTN published standardized definitions of AOOS to guide future data analysis, policy development, and oversight. Input from the Data Advisory Committee (DAC) and the Patient Affairs Committee (PAC) was essential in shaping the AOOS definitions, ensuring transparency and meaningful engagement across the transplant community.
Coming soon:
- The AOOS Workgroup will develop a 90-day action plan for implementing the most critical components of the Plan, such as educating OPTN members on current allocation policies; evaluating OPTN member compliance; and developing an administrative definition for the "offer" of an organ by an OPO to a transplant center.
- New compliance criteria will be introduced to audit the use of "Other, specify" organ offer refusal and bypass codes (e.g., 799). Bypass codes document why a patient was skipped instead of receiving an offer. Each use of an “Other, specify” code will require documented justification, helping to reduce misclassification and improve policy adherence. Updated policies will reinforce accountability and ensure appropriate use of bypass reasons.
This website will be updated regularly with progress, data trends, and other relevant information.
What has been communicated between HRSA and the OPTN?
Transparency and oversight are foundational to how HRSA is addressing AOOS. Since August 2024, HRSA and the OPTN have collaborated to define AOOS, address compliance gaps, and develop an actionable remediation plan. Visit the OPTN Critical Comments web page for a full summary of AOOS communications between HRSA and the OPTN.
Stay up to date

- Monthly updates: HRSA OPTN Modernization initiative
- Policy Comments: Public Comment Page
- AOOS Critical Comments & Responses: Critical Comments Archive
- Staying compliant: What You Need to Know About AOOS